

The Australian Transport Safety Bureau (ATSB) has concluded that poor bridge resource management (BRM), communication breakdowns, and procedural lapses led to the collision between the 333-meter container ship Maersk Shekou and the tall ship STS Leeuwin II in Fremantle Port, Western Australia, on August 30, 2024.
The incident occurred under heavy squall conditions and resulted in substantial damage to the Leeuwin II, minor injuries to two of its crew, and a hull breach on the Maersk Shekou.
Circumstances of the incident
In the early morning hours, the Maersk Shekou, under the Singapore flag, was inbound to Fremantle’s inner harbor with two pilots on the bridge and four assist tugs assigned.
Winds gusted up to 50–54 knots, exceeding the port’s normal operational limits. As the vessel approached the inner harbor entrance channel, it encountered a strong southwesterly squall on its starboard quarter. Despite the helmsman applying 30 degrees of port rudder, the ship’s heading could not be maintained.
At the designated wheel-over point near South Mole, the pilot failed to issue a 10-degree port helm order to initiate the turn into the harbor. The helmsman, following the last instruction to steer 083°, maintained that heading straight toward Victoria Quay – where the Leeuwin II was moored. The omission went unnoticed by the bridge team.
Collision and immediate consequences
At approximately 06:18, despite the pilots’ efforts to correct course using engine and tug commands, the Maersk Shekou’s starboard bow flare struck the rigging of the Leeuwin II, dismasting the historic vessel.
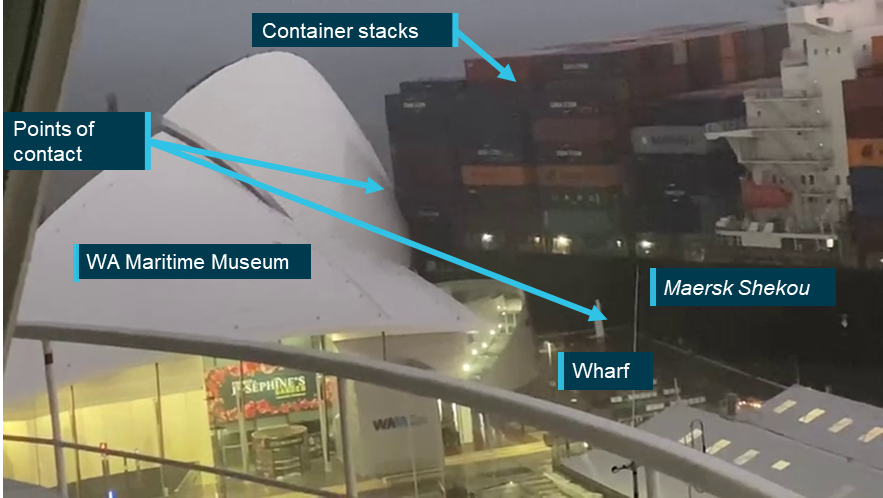
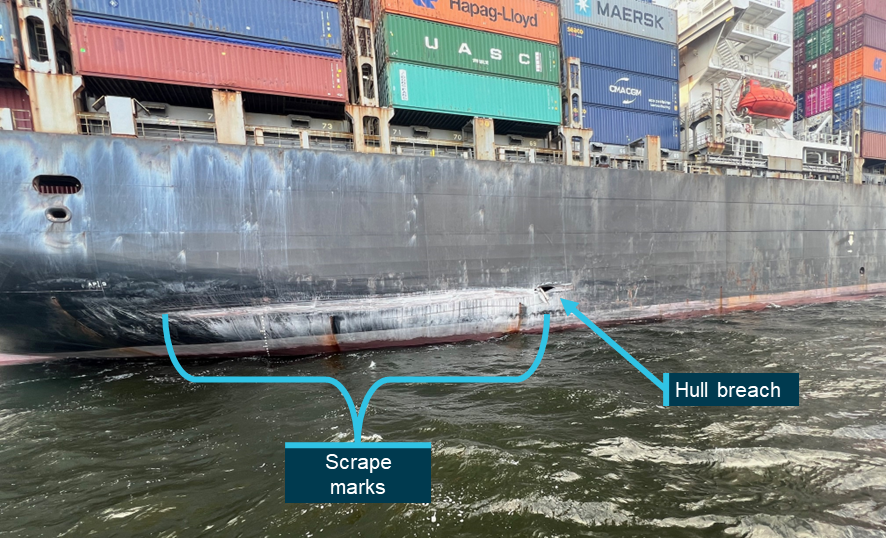
The Leeuwin II’s crew evacuated to the pier moments before impact, with two sustaining minor injuries while escaping down the gangway. The container ship’s stern continued swinging toward the pier, causing containers stacked on its poop deck to strike the roof of the Western Australian Maritime Museum. A hull breach roughly six feet long was later found above the waterline.
Findings of the ATSB investigation
The ATSB identified several key contributing factors:
1. Ineffective bridge resource management
- The bridge team – including the two pilots and ship’s officers – failed to actively monitor the ship’s rate of turn, helm, and position.
- There was no shared mental model among team members regarding wheel-over points and course alterations.
- Errors were neither challenged nor corrected early, reflecting poor coordination and situational awareness.
2. Distraction during critical passage
- The secondary pilot was engaged in a non-essential mobile phone call during the approach to the inner harbor.
- This distraction prevented timely detection that the lead pilot had omitted the course alteration and that the helmsman’s steering opposed the intended maneuver.
3. Procedural non-compliance and risk oversight
- The vessel entered the inner harbor before sunrise and with not all tugs yet made fast – both violations of Fremantle Ports’ documented safety procedures.
- Wind conditions exceeded established operational limits, yet no formal reassessment of the risks was conducted before the abort point.
- Several of the port’s risk controls for large container vessel entries were inconsistently applied or ineffective, including daylight-only restrictions, wind thresholds, and communication between Vessel Traffic Services (VTS) and pilots.
4. Increased workload and poor task management
- The fourth tug was still being made fast during the critical turning phase, adding unplanned workload and distraction to the bridge team.
- The helmsman did not promptly report difficulty in maintaining course, delaying corrective action.
Additional risk factors
The ATSB highlighted further operational weaknesses that, while not directly causal, increased the likelihood of an accident:
- Ineffective monitoring role of the secondary pilot.
- Inconsistent procedural documentation regarding tug usage and operational parameters.
- Insufficient communication between pilots and VTS concerning weather updates and evolving conditions.
- Inadequate challenge-response culture within the bridge team, preventing early identification of errors.
Lessons and safety recommendations
The investigation underscored the critical importance of effective BRM and communication discipline on the bridge:

“A properly functioning bridge team requires that all its members maintain a shared mental model to actively monitor the ship’s progress. To ensure this is effective, where deviations from the passage plan are required, this information should be conveyed to all members of the team. Similarly, actions that are incorrect or missed should be immediately identified, communicated and rectified,” ATSB stated.
Both Fremantle Ports and pilotage provider Fremantle Pilots have since committed to implementing corrective safety actions, including:
- Strengthening monitoring protocols and communication standards during pilotage operations.
- Reinforcing adherence to operational limits for wind and daylight restrictions.
- Enhancing pilot training and fatigue management.
As the ATSB emphasized, minimizing distractions, maintaining situational awareness, and fostering a cohesive bridge team culture are vital defenses against future navigational casualties.














