
A serious injury on board the survey vessel serves as a stark reminder of how quickly routine operations can go wrong. The second officer sustained crush injuries to his lower left leg when it became caught in a rail-mounted deck crane’s rack and pinion mechanism during a lifting operation. The Nautical Institute highlighted this case to illustrate the dangers of using crane controls contrary to the manufacturer’s instructions and to show how unsafe practices, once normalised for convenience, can have catastrophic consequences.
Incident overview
A survey/supply vessel was preparing for a contract requiring the movement of several heavy items of deck equipment and machinery. A lifting plan and permit to work were completed, and the deck crew was briefed on the tasks ahead.
A deck officer and a fitter went on deck to move the items using the starboard rail-mounted crane. The officer climbed the ladder to access the crane and operated it using the local hydraulic controls on the crane pedestal – the only method he knew, learned during his arrival familiarisation training.
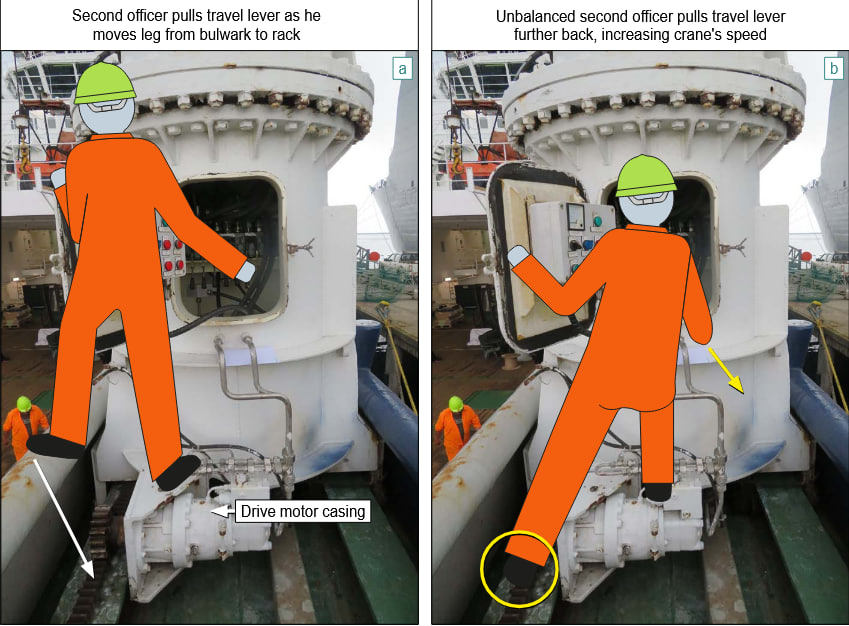
After repositioning two loads on the main deck, they began a third lift. To see both the fitter and the load 4 m below on the deck, the officer stood with his left foot on the inboard bulwark and his right foot on the crane drive. When shifting his left foot to the crane’s travel rack, he felt something pull at his overalls, which unbalanced him.
He grabbed the crane travel lever for stability, unintentionally increasing the speed of the crane traverse. His left leg was pulled into the rack and pinion drive. Releasing the lever stopped the crane.
The fitter climbed to the crane’s rail and found the officer lying on his back, his left leg trapped. Following the officer’s instructions to move the crane forward, the fitter freed the leg, which was severely mangled below the knee. The vessel’s first-aid team responded immediately, and the injured officer was evacuated by helicopter to hospital, where a below-knee amputation was required.
Investigation findings
The crane manufacturer’s manual, available on board, clearly stated that the local pedestal controls were for emergency use only. Normal operation was to use either the bridge control station or the crane’s remote-control unit.
The company’s Safety Management System (SMS) lacked ship-specific operating instructions. The practice of operating the crane at height without guardrails or restraints, and near exposed rack and pinion gearing, revealed serious procedural flaws.
Although the crew had the freedom to challenge unsafe practices on board, they considered the use of local controls “normal” and did not question it. This demonstrated both a disregard for manufacturer instructions and a tolerance of unsafe acts and conditions.
Lessons learned
- Recognize hazards consciously: Hazards in familiar areas are not always obvious. Always look at each task with fresh eyes. Ask yourself – could this be dangerous?
- Ship-specific procedures are essential: Generic SMS instructions are only the first layer of protection. Each vessel should have procedures tailored to its specific layout, equipment, and risks. The crew, who know the ship best, should actively develop these procedures.














